Cardiac Index
Cardiac Index calculator assesses cardiac output relative to body surface area, providing a measure of cardiac function indexed to body size. It is useful for evaluating cardiac performance in critically ill patients.
Inputs
Result
Enter values to calculate
Formula
CI = CO / BSA📚 Calculator References(3)
Theory and Practice
Physiological Basis
The cardiac index is a hemodynamic parameter that relates the cardiac output to body surface area, providing a more individualized assessment of cardiac function. Consider how, as with other hemodynamic measurements, a cardiac output of, for example, 4L/min can mean very different things for a 50kg woman as opposed to a 120kg man. For a smaller adult, 4L/min may be a high cardiac output, which in the context of shock may indicate a more distributive picture compared to the 120kg man whose normal cardiac output is 5-6L/min. For the larger adult, 4L/min being a low cardiac output indicating a cardiac component to their shock state. Taken without the appropriate patient context, non-indexed cardiac output alone lacks the nuance to accurately characterize a patients shock state.
Clinical Application
Whether cardiac output was derived non-invasively via VTI, Fick, or a pulmonary artery catheter and theromodilution, all of these values can be adjusted for body surface area to obtain a cardiac index. In critically ill patients, we know that shock states rarely stay within their standalone pillars of cardiogenic, distributive, hypovolemic and so on. A patient with septic shock may have low cardiac output from septic cardiomyopathy or pre-existing heart failure with reduced ejection fraction, or a patient with hemorrhagic shock may develop stress cardiomyopathy during their resuscitation leading to reduced cardiac output.
When patients are not improving, have pre-existing impaired cardiac function, or shock is suspected to be mixed, obtaining a cardiac index provides an objective measure of cardiac sufficiency.
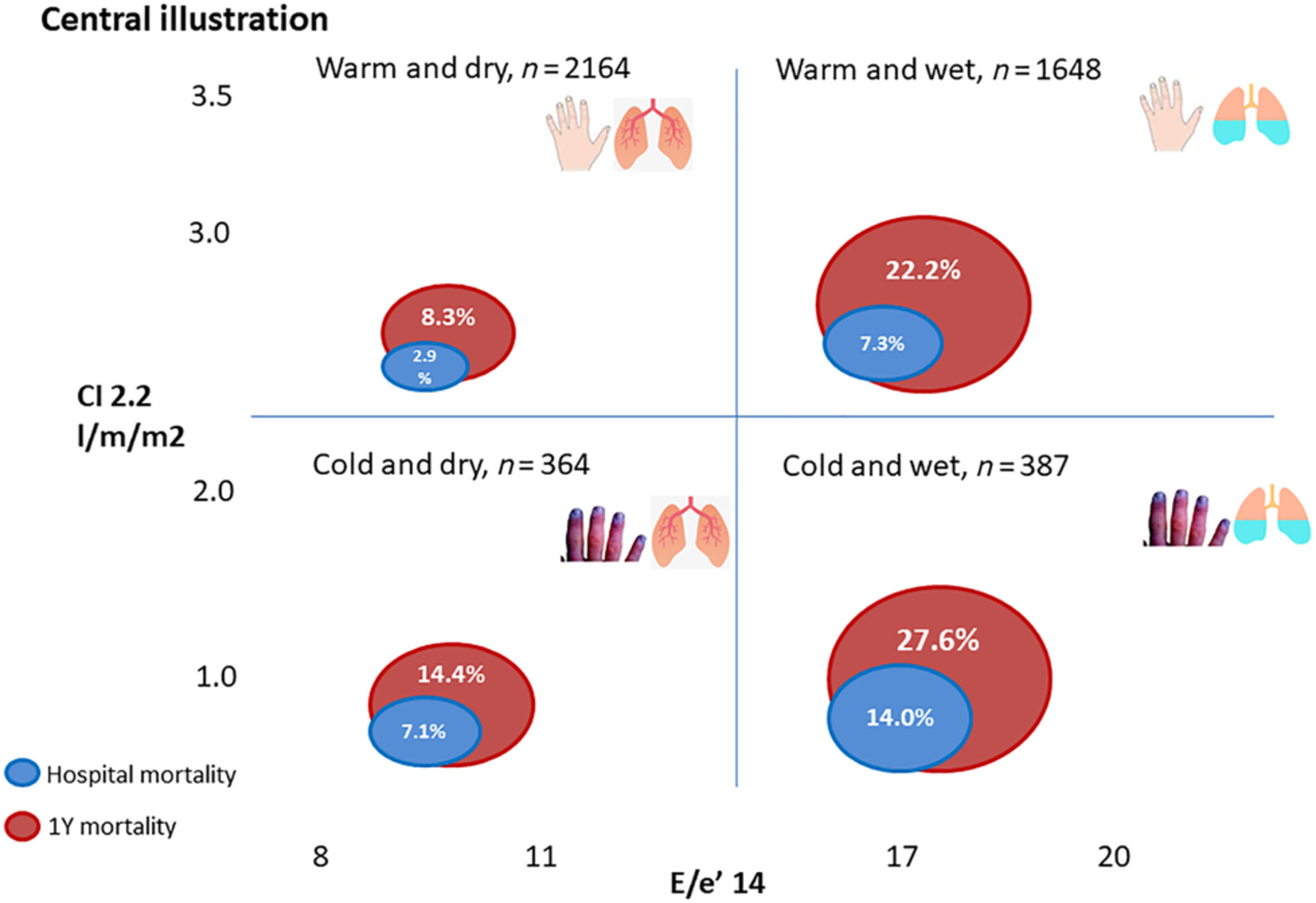
Classically, the hemodynamic definition of cardiogenic shock is a cardiac index <2.2L/min/m2 . For pure cardiogenic shock, anything beyond SCAI-C has by definition an index <2.2. Remember that other shock states may lead to low cardiac index - hemorrhagic shock or pulmonary embolism for example will have low cardiac index due to inadequate left ventricular preload.
If you have a patient with shock and a low cardiac index, consider the broader picture of their other hemodynamic parameters to assess if there is a significant cardiac component to their shock. Do they have an elevated wedge pressures, or a high systemic vascular resistance index consistent with cardiogenic shock? Will they benefit from inotropy, or mechanical circulatory support? If you suspect shock is has a significant cardiac component, reassess after initiating inotropy and vasodilators their cardiac index again! Has improving their cardiac index improved their shock/markers of perfusion?
Evidence Base
Numerous studies have validated the use of cardiac index in assessing cardiac function and guiding treatment in critically ill patients. This dates back to the era before coronary reperfusion, where the Diamond and Forrester classification used cardiac index and pulmonary wedge capillary pressure to prognosticate post-myocardial infarction mortality.
Translating this more broadly to the cardiogenic shock literature, cardiac index is one of the most sensitive predictive markers of mortality in cardiogenic shock, with an index of <1.8L/min/m2 in the first 24 hours of shock being a sensitive indicator for mortality. Beyond predictors of mortality, CI also provides a useful target when assessing effective treatment. Retrospective cohort studies have shown that an ability to increase cardiac index >3.0 improves mortality when compared to >2.0 and 2.5, suggesting that an ability to increase CI more than just >2.2 may be beneficial.
In septic shock, cardiac index also plays an important role as values at either extreme (low cardiac index indicating a cardiogenic component, or high cardiac index indicating significant vasoplegia) are associated with increased mortality in a U shaped curve. While septic shock is a complex pathophysiologic process with microcirculatory dysfunction, septic microthrombi, and endothelial dysfunction, ensuring an adequate cardiac index and changes to cardiac index with fluid responsiveness testing may provide additional treatment strategies to assist in end organ perfusion.
References
- 1. Torgersen C, Schmittinger CA, Wagner S, Ulmer H, Takala J, Jakob SM, Dünser MW. Hemodynamic variables and mortality in cardiogenic shock: a retrospective cohort study. Crit Care. 2009;13(5):R157. doi: 10.1186/cc8114. Epub 2009 Oct 2. PMID: 19799772; PMCID: PMC2784383.
- 2. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation. 2017. van Diepen S, Katz JN, Albert NM, et al.
- 3. Monnet X, Messina A, Greco M, Bakker J, Aissaoui N, Cecconi M, Coppalini G, De Backer D, Edul VK, Evans L, Hernández G, Hunsicker O, Ince C, Kaufmann T, Levy B, Malbrain MLNG, Mebazaa A, Myatra SN, Ostermann M, Pinsky MR, Saugel B, Savi M, Singer M, Teboul JL, Vieillard-Baron A, Vincent JL, Chew MS. ESICM guidelines on circulatory shock and hemodynamic monitoring 2025. Intensive Care Med. 2025 Nov;51(11):1971-2012. doi: 10.1007/s00134-025-08137-z. Epub 2025 Nov 14. PMID: 41236566.
- 4. Kim, K.-H., Jentzer, J. C., Wiley, B. M., Miranda, W. R., Bennett, C., Barsness, G. W., and Oh, J. K. (2021) Diamond–Forrester classification using echocardiography haemodynamic assessment in cardiac intensive care unit patients. ESC Heart Failure, 8: 4933–4943
- 5. Levy B, Curtiaud A, Duarte K, Delmas C, Demiselle J, Girerd N, Gebhard CE, Helms J, Meziani F, Kimmoun A, Merdji H. Association between mean hemodynamic variables during the first 24 h and outcomes in cardiogenic shock: identification of clinically relevant thresholds. Crit Care. 2025 Mar 26;29(1):137. doi: 10.1186/s13054-025-05356-0. PMID: 40140876; PMCID: PMC11948639.
- 6. Ngan C, Zeng X, Lia T, Yin W, Kang Y. Cardiac index and heart rate as prognostic indicators for mortality in septic shock: A retrospective cohort study from the MIMIC-IV database. Heliyon. 2024 Apr 1;10(8):e28956. doi: 10.1016/j.heliyon.2024.e28956. PMID: 38655320; PMCID: PMC11035949.
Contributors

Isaac Bonisteel

Dr. Ross Prager