Mean Arterial Pressure (MAP) Calculator
This calculator is used to determine the average blood pressure within the arteries, which is important for perfusion of organs.
Inputs
Result
Enter values to calculate
Formula
MAP = (2 * DBP + SBP) / 3 Theory and Practice
Mean arterial pressure (MAP) is the average pressure throughout arterial circulation over the course of the cardiac cycle. It can be expressed as the product of cardiac output and systemic vascular resistance, or estimated clinically as the time-weighted mean of the arterial pressure waveform.
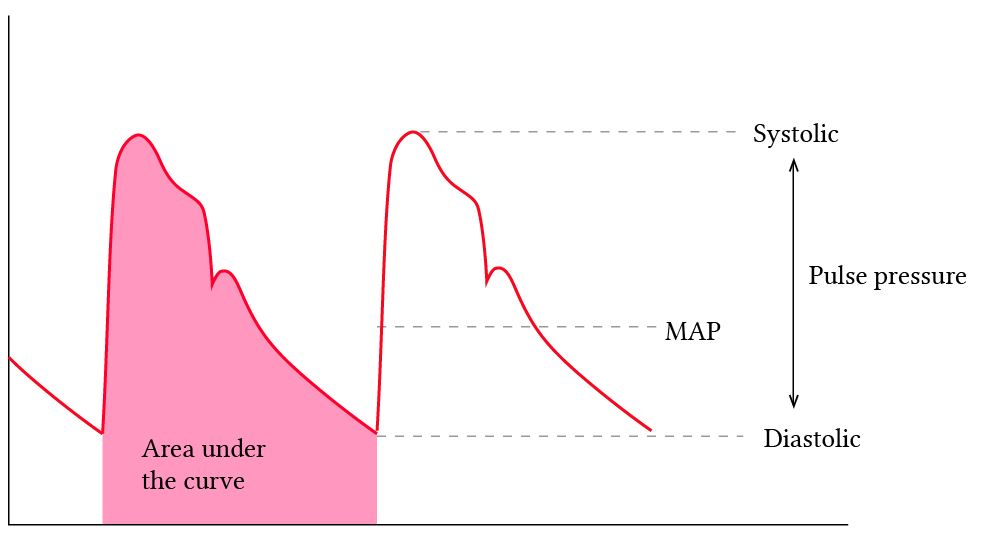
MAP is appealing because it is less susceptible to measurement artifacts than systolic or diastolic pressures and aligns with key physiologic mechanisms, including organ autoregulation and baroreceptor function. Consider how an arterial line, if over or under dampened, may provide inadequate systolic and diastolic pressures but the MAP will remain accurate (in the above diagram, systolic and diastolic pressures may vary, but the area under the curve will remain the same.
In practice, MAP has become the "North Star" of resuscitation, with 65 mmHg often cited as the minimum target for adequate perfusion. This value, however, rests more on consensus than strong evidence.
The 65 Trial (Lamontagne et al., 2020) showed that targeting a lower range (60–65 mmHg) in older patients with vasodilatory shock reduced vasopressor exposure without increasing mortality, and may even be protective in some subgroups.
Conversely, ANDROMEDA-SHOCK-2 demonstrated that a MAP of 65 may be inadequate for perfusion if there is low stroke volume, or extremely low diastolic pressure (less than 50mmHg).
Studies looking at higher MAP targets (>80mmHg) in septic shock (SEPSISPAM, OPTPRESS) have shown mixed evidence on mortality and end organ perfusion). These mixed results highlight the variable phenotypes of broad overarching processes like septic shock, and how more personalized assessments and interventions are likely beneficial.
Two recent meta-analyses assessed the effect of targeting higher vs lower MAP targets in various shock phenotypes; the first in 2023 by Carayannopoulos et al. not showing any significant difference in mortality, but a possible reduced need for renal replacement therapy in the higher MAP arm. The second meta-analysis released in 2025 by Mendes et al. showed an increased mortality risk associated with targeting a higher MAP, largely because of the findings of OPTPRESS. These studies aren't perfect, they do not account for variability in shock phenotypes, and are limited in practice by adherence to target MAPs.
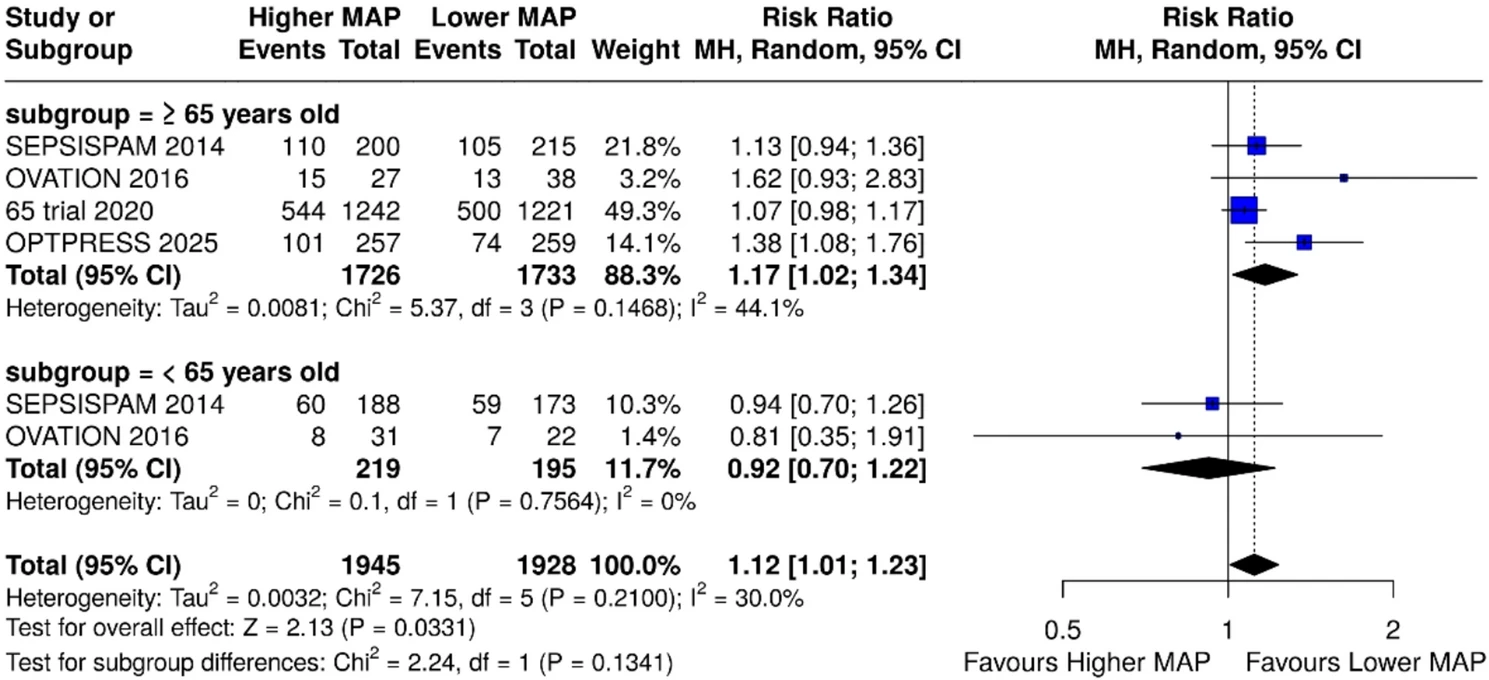
When grouped, there are however some interesting trends we can see in patient related outcomes. Consider the trend towards improved mortality in in targeting a lower MAP when patients aged >65 are pooled together (see right). This makes us question an interesting physiologic concept that is the basis for targeting higher MAPs - the premise that those with hypertension (a common comorbidity in those aged >65) may require a higher MAP to receive adequate perfusion.
Generally, the variability and lack of reproducibility of MAP trials suggests that there is more to perfusion in shock than targeting numbers. Inadequate MAP can certainly contribute to microcirculatory dysfunction, particularly in the presence of low flow states or venous congestion (Hemodynamic Interfaces Calculator). For this reason, MAP should be interpreted in context: as one piece of a broader hemodynamic assessment that incorporates patient comorbidities, perfusion endpoints, and individualized goals, rather than a rigid target applied universally.
References
- 1. Asfar P, Meziani F, Hamel JF, Grelon F, Megarbane B, Anguel N, Mira JP, Dequin PF, Gergaud S, Weiss N, Legay F, Le Tulzo Y, Conrad M, Robert R, Gonzalez F, Guitton C, Tamion F, Tonnelier JM, Guezennec P, Van Der Linden T, Vieillard-Baron A, Mariotte E, Pradel G, Lesieur O, Ricard JD, Hervé F, du Cheyron D, Guerin C, Mercat A, Teboul JL, Radermacher P; SEPSISPAM Investigators. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014 Apr 24;370(17):1583-93. doi: 10.1056/NEJMoa1312173. Epub 2014 Mar 18. PMID: 24635770.
- 2. The ANDROMEDA-SHOCK-2 Investigators for the ANDROMEDA Research Network, Spanish Society of Anesthesiology, Reanimation and Pain Therapy (SEDAR), and Latin American Intensive Care Network (LIVEN). Personalized Hemodynamic Resuscitation Targeting Capillary Refill Time in Early Septic Shock: The ANDROMEDA-SHOCK-2 Randomized Clinical Trial. JAMA. 2025;334(22):1988–1999. doi:10.1001/jama.2025.20402
- 3. Endo A, Yamakawa K, Tagami T, Umemura Y, Wada T, Yamamoto R, Nagasawa H, Takayama W, Yagi M, Takahashi K, Kojima M, Narita C, Kazuma S, Takahashi J, Shiraishi A, Todani M, Nakane M, Nagata T, Tanaka S, Yokokawa Y, Takahashi K, Ishikita H, Hisamune R, Sasaki J, Muramatsu KI, Sonobe H, Minami K, Hoshi H, Otomo Y; OPTPRESS trial investigators. Efficacy of targeting high mean arterial pressure for older patients with septic shock (OPTPRESS): a multicentre, pragmatic, open-label, randomised controlled trial. Intensive Care Med. 2025 May;51(5):883-892. doi: 10.1007/s00134-025-07910-4. Epub 2025 May 13. PMID: 40358717; PMCID: PMC12130109.
- 4. Carayannopoulos, Kallirroi Laiya MD, FRCPC1; Pidutti, Andrew BSc2; Upadhyaya, Yashita MD1; Alshamsi, Fayez MD, FRCPC3; Basmaji, John MD, FRCPC4; Granholm, Anders MD5; Alhazzani, Waleed MD, MSc, FRCPC1,6; Lewis, Kimberley MD, MSc, FRCPC1,6. Mean Arterial Pressure Targets and Patient-Important Outcomes in Critically Ill Adults: A Systematic Review and Meta-Analysis of Randomized Trials*. Critical Care Medicine 51(2):p 241-253, February 2023. | DOI: 10.1097/CCM.0000000000005726
- 5. Mendes, H., King, J., Kumar, N. et al. Mortality effect of higher versus lower blood pressure targets in vasodilatory shock: an updated systematic review and meta-analysis. Crit Care 30, 17 (2026).
Contributors

Dr. Ross Prager

Caseng Zhang

Isaac Bonisteel